Orbital
Anophthalmos
Surgical and prosthetic management of anophthalmos (absence of the eye) and socket reconstruction following enucleation or evisceration.
Medically reviewed by Noel D. Saks, MDOculoplastic SurgeonLast updated June 2026
Orbital
Surgical and prosthetic management of anophthalmos (absence of the eye) and socket reconstruction following enucleation or evisceration.
Medically reviewed by Noel D. Saks, MDOculoplastic SurgeonLast updated June 2026
Anophthalmos (or anophthalmia) refers to the absence or loss of the eye within the orbit. The term covers a broad spectrum — from congenital absence of the globe, to acquired loss of the eye from trauma, tumor, or advanced ocular disease. Regardless of cause, the result is an empty or shrunken socket that requires reconstruction to restore volume, support a prosthesis, and maintain a natural facial appearance.
Modern orbital implants and socket-reconstruction techniques have transformed outcomes for patients with anophthalmos. ASOPRS-trained oculoplastic surgeons provide orbital implant surgery, socket reconstruction, and long-term prosthetic management for patients of all ages — including children with congenital conditions who need stimulation of orbital growth.
Congenital anophthalmos is classified by the stage at which ocular development failed:
True primary anophthalmos is very rare; extreme microphthalmos (a very small globe within the orbital soft tissue) is more commonly encountered clinically. Anophthalmos and microphthalmos can occur as isolated findings or as part of syndromes associated with chromosomal abnormalities, including Trisomy 13.
Congenital anophthalmos may result from inherited or sporadic genetic mutations, chromosome abnormalities, prenatal environmental insults (infections, teratogens), or unknown causes. Development of the eyelids, conjunctival fornices, and bony orbit depends on the presence of a normal-sized eye during fetal growth; absence or severe reduction of the globe impairs orbital development and requires early intervention.
Acquired anophthalmos results from surgical removal of the eye for trauma (severe injury not amenable to repair), tumor (retinoblastoma, choroidal melanoma, other intraocular malignancies), infection (endophthalmitis unresponsive to treatment), or advanced ocular disease (end-stage glaucoma, a painful blind eye).

When the eye cannot be saved, two primary procedures are available:
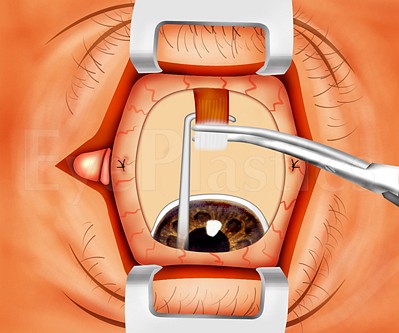
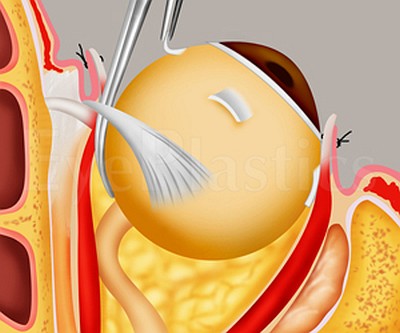
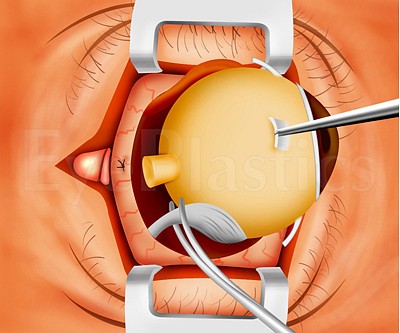
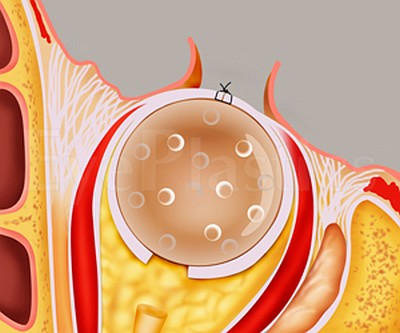
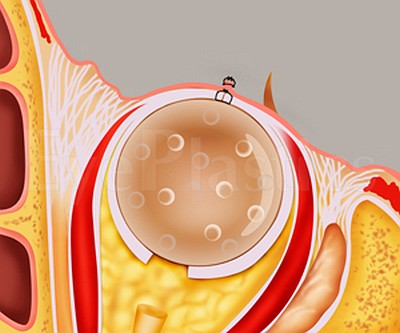
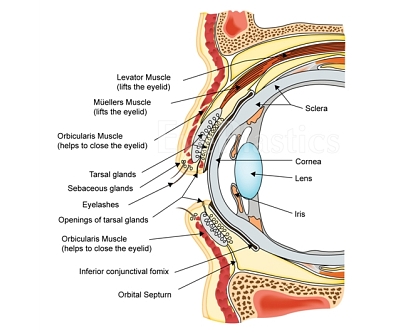
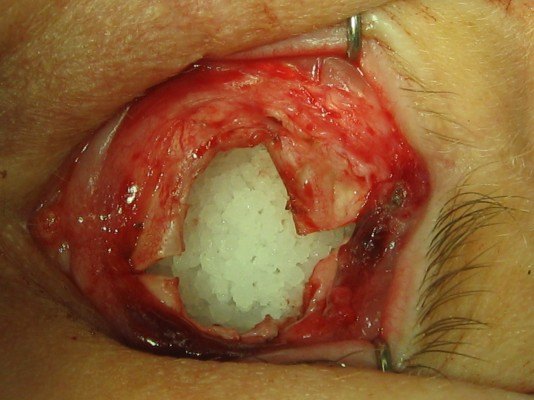
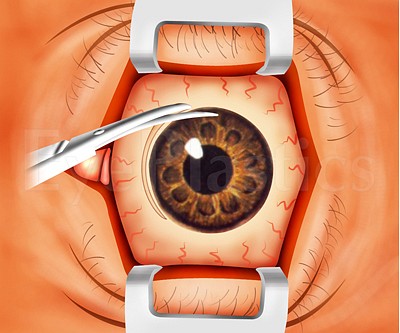
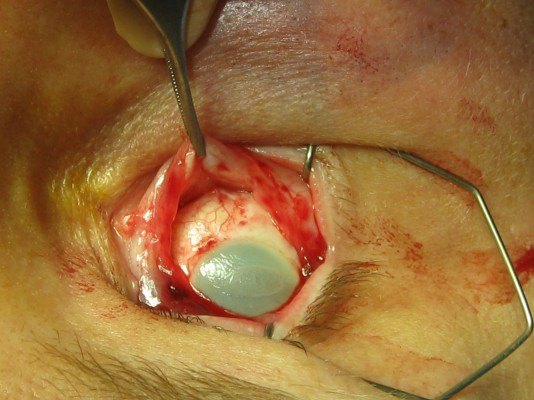
Following either procedure, an orbital implant is placed within the muscle cone to restore orbital volume, and a custom ocular prosthesis is fitted by an ocularist 4–6 weeks later. The animations below illustrate the relevant anatomy and both procedures step by step.
Choose a procedure, then drag the slider to step through it.
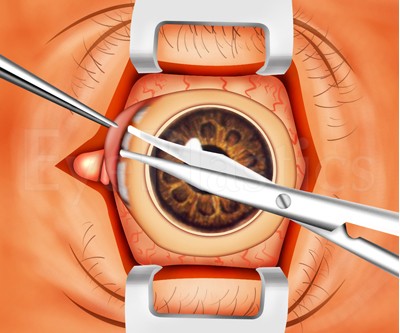
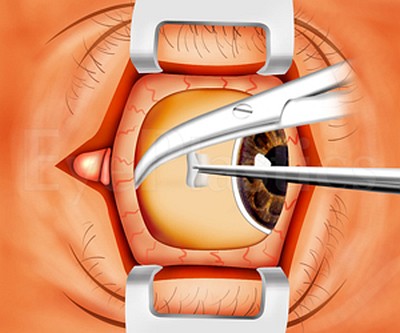
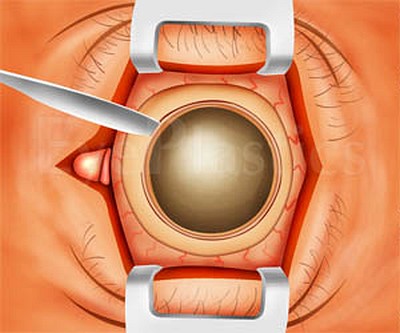
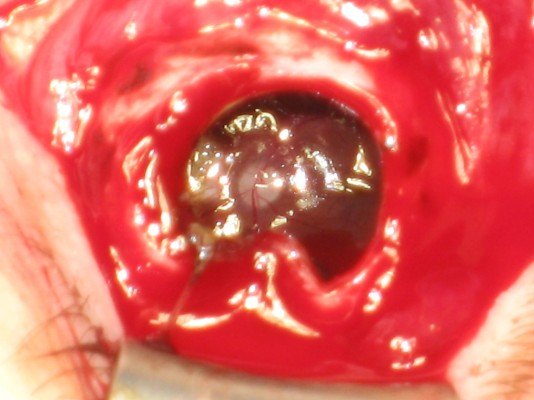
Step 1 of 16
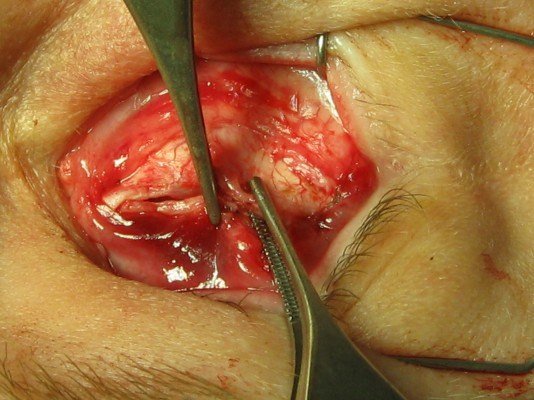
The eye is exposed, ready for surgery
Drag the slider to compare
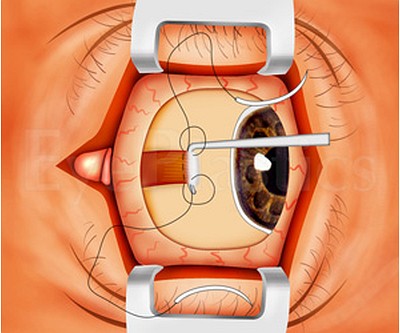
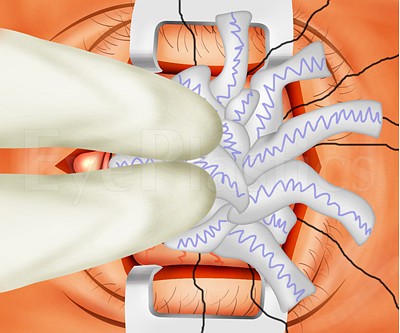
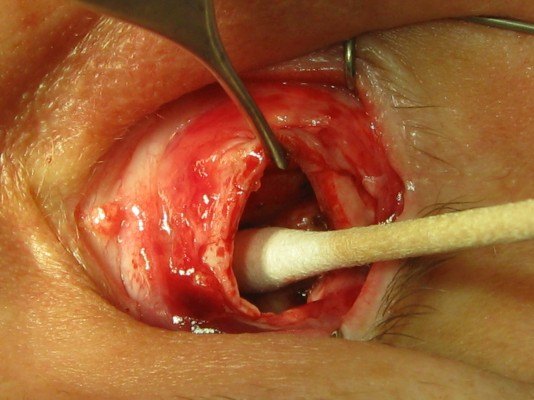
Step 1 of 15
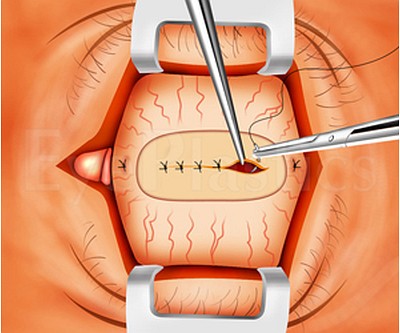
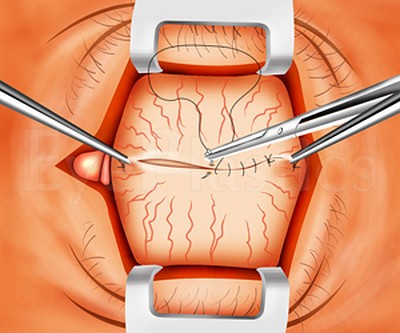
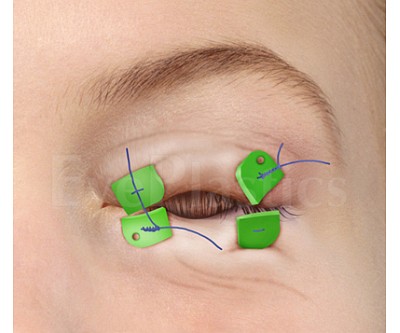
Opening the conjunctiva
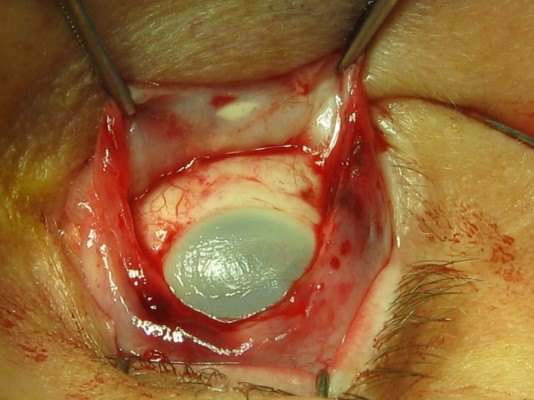
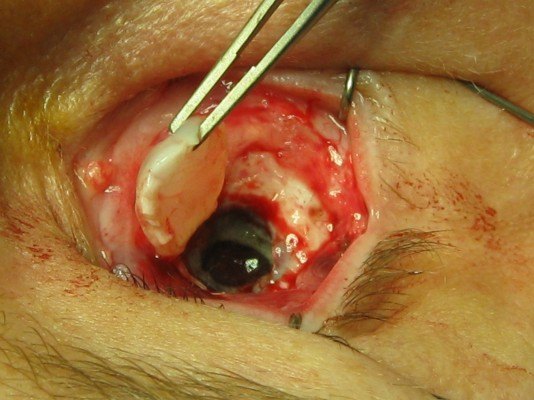
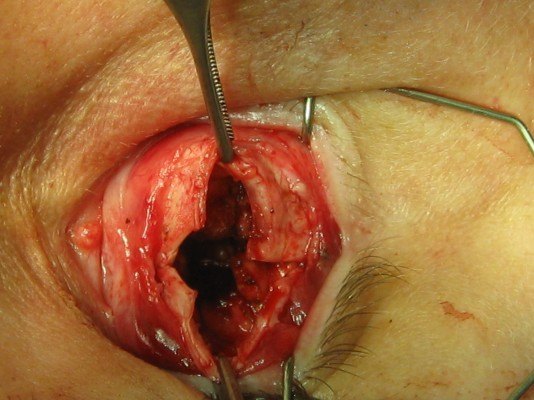
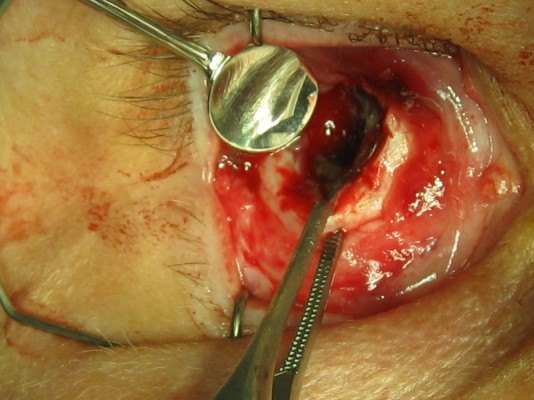
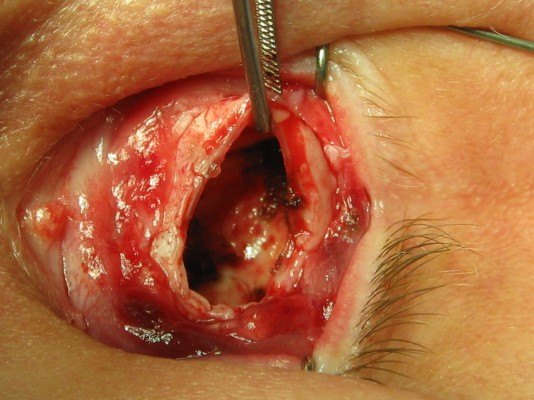
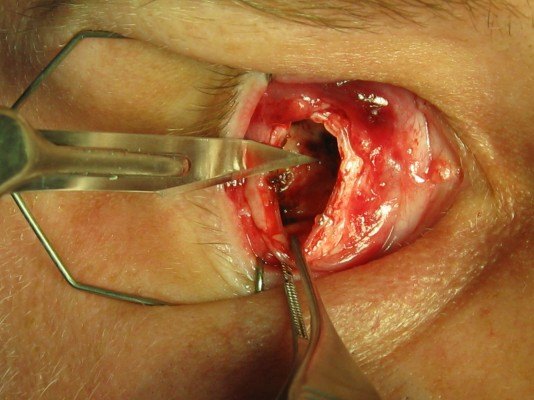
Drag the slider to step through the evisceration technique. These are real surgical images.
How orbital implants restore volume and movement after the eye is removed.
Retinoblastoma is the most common primary intraocular malignancy of childhood, arising from the developing retina and usually diagnosed before age five. It is one of the most important reasons an eye is removed in a child, and the oculoplastic and ocularist team plays a central role in reconstructing and maintaining the socket as the child grows.
Early sign — leukocoria. A white pupillary reflex (a white rather than red “red-eye” in flash photographs), a new eye turn (strabismus), or a red, painful eye in a young child should prompt urgent ophthalmology referral.
Genetics & presentation
Diagnosis & staging
Eye-sparing treatment is the goal whenever the eye and useful vision can be saved — systemic or intra-arterial chemotherapy (chemoreduction), focal laser, cryotherapy, and plaque brachytherapy are used for less advanced tumors, ideally at a specialized ocular-oncology center.
When enucleation is indicated. Removal of the eye is recommended for advanced unilateral disease, when there is no prospect of useful vision, or when sparing the eye would risk spread of the tumor — particularly along the optic nerve. Two principles guide the surgery:
Because the orbit is still growing, children with an anophthalmic socket need ongoing follow-up; a well-fitted, regularly upgraded prosthesis (and avoidance of unnecessary radiation when possible) helps the bony orbit and lids develop symmetrically. With early detection and modern treatment, survival in developed countries exceeds 95%, which is why recognizing leukocoria early is so important. Pathology and any need for additional chemotherapy or radiation are coordinated with pediatric oncology.
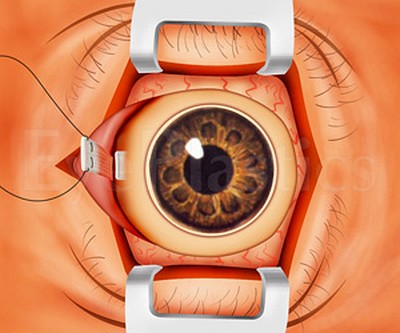
A custom ocular prosthesis (artificial eye) is fitted over the healed implant by a certified ocularist, who hand-paints it to match the fellow eye’s iris, limbus, and scleral vessels. The sequence below shows the progression from the healed socket to a fitted prosthesis.




Schedule a consultation with Noel D. Saks, MD to learn if this procedure is right for you.