Part of our complete guide to Thyroid Eye Disease (TED) — this page covers TED diagnosis and evaluation in depth.
Thyroid eye disease is recognized by a characteristic set of eye findings and graded by how active and how severe it is. This page covers the clinical signs, the orbital imaging, and the scoring systems used to guide treatment.
Eye Signs of Thyroid Eye Disease
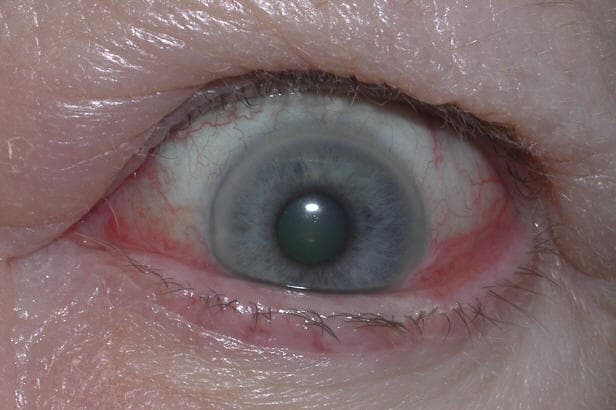
The hallmark findings of TED include proptosis, lid retraction, restricted eye movement, and periorbital swelling. The combination of these features gives the characteristic “staring” or “startled” appearance.
Clinical Findings
Proptosis (exophthalmos): Forward displacement of the globe due to expanded orbital volume. Hertel exophthalmometry readings > 21 mm, or ≥ 2 mm of asymmetry between the eyes, are considered significant (normal values vary by ethnicity). Thyroid eye disease is the most common cause of proptosis in adults, and is also the most common cause of bilateral proptosis
Eyelid retraction: Upper lid scleral show (limbus to upper lid margin >2 mm) and lower lid scleral show below the limbus. Both sympathetic over-stimulation and levator fibrosis contribute
Restrictive strabismus: Tight, fibrotic extraocular muscles restrict movement and cause diplopia, most commonly on upgaze (inferior rectus) and lateral gaze (medial rectus)
Periorbital edema and chemosis: Inflammatory swelling of eyelids, conjunctiva, and caruncle
Corneal exposure keratopathy: Incomplete eyelid closure and reduced blink rate from proptosis and lid retraction expose the cornea — causing dryness, pain, and risk of corneal ulceration
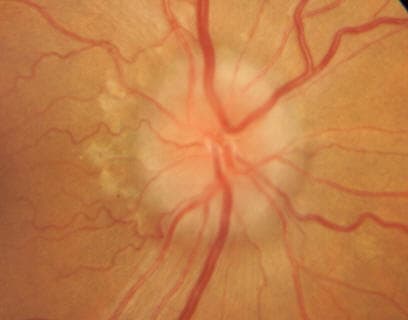
Compressive optic neuropathy (CON): The most vision-threatening complication — enlarged muscles at the orbital apex compress the optic nerve. Presents with decreased visual acuity, color desaturation, and relative afferent pupillary defect. Requires urgent treatment
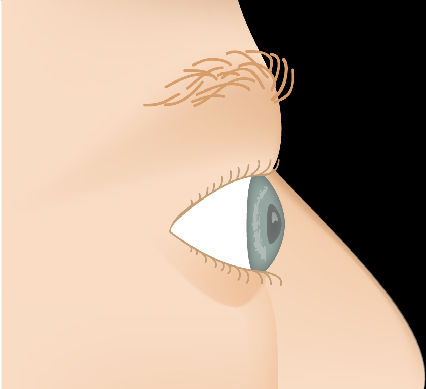
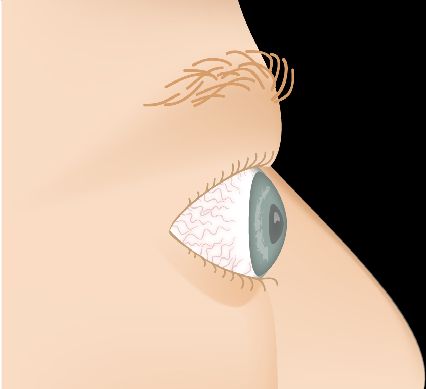
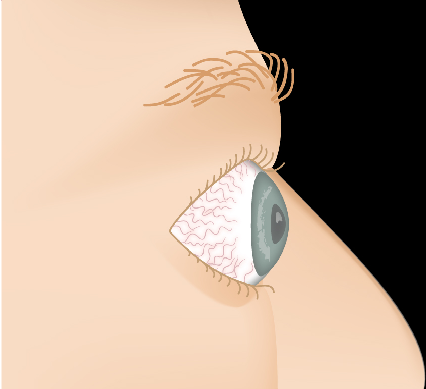
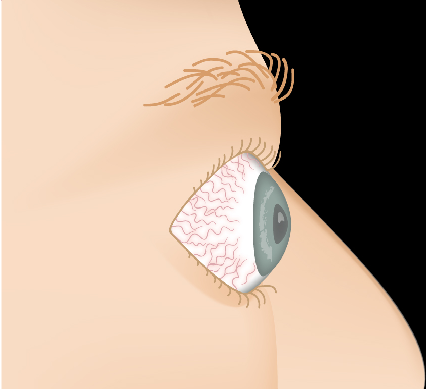
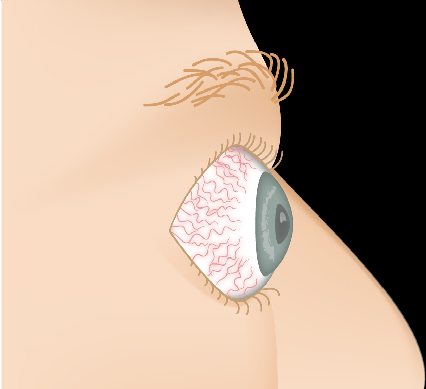
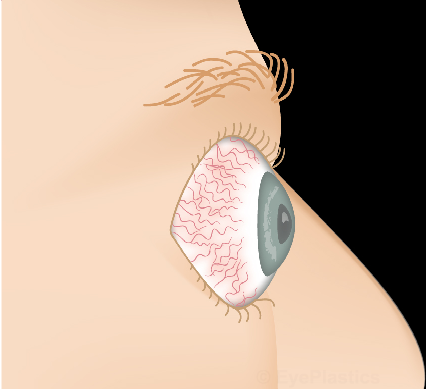
ProptosisOrbital Changes
Interactive visualization showing orbital muscle changes and progressive proptosis associated with Thyroid Eye Disease.
HealthyAdvanced
Drag the slider to compare
Radiological Findings
CT of the orbits characteristically demonstrates enlarged extraocular muscles (particularly inferior and medial rectus) with sparing of the tendinous insertions — a key feature distinguishing TED from orbital myositis, where the tendon is involved. Crowding of the enlarged muscles at the orbital apex (apical crowding) predicts risk of optic neuropathy.
Disease Activity & Severity
TED has two distinct phases: an active (inflammatory) phase of variable duration (typically 6–24 months) followed by an inactive (fibrotic) phase. Timing of treatment is critical — most medical therapies work only during the active phase.
Clinical Activity Score (CAS)
The CAS assigns one point for each of the following signs of active inflammation:
Spontaneous orbital pain
Pain on eye movement
Eyelid erythema
Conjunctival injection
Chemosis
Swelling of the caruncle or plica
Eyelid edema
A CAS ≥ 3/7 indicates active disease. Active disease may respond to medical therapy such as corticosteroids and the IGF-1R inhibitor teprotumumab (Tepezza); teprotumumab requires monitoring for hearing impairment and hyperglycemia; it can harm a developing fetus, so it must not be used in pregnancy and effective contraception is required during treatment and for 6 months after the final dose; inactive disease does not — surgical rehabilitation is the appropriate approach for stable inactive TED.
Severity Classification
Mild TED
Minimal impact on quality of life
Lid retraction < 2 mm
Proptosis < 3 mm above normal
Mild corneal exposure
Transient or no diplopia
Managed conservatively; observation is appropriate
Moderate-to-Severe TED
Significant impact on daily life
Lid retraction ≥ 2 mm
Proptosis ≥ 3 mm above normal
Intermittent or constant diplopia
Corneal exposure requiring treatment
Active disease is usually treated with teprotumumab (Tepezza) or IV corticosteroids, individualized to the patient
Sight-threatening TED: Compressive optic neuropathy or severe corneal exposure requires urgent treatment — urgent high-dose IV corticosteroids and/or orbital decompression surgery regardless of disease phase. Any sudden decrease in vision, dimming of color, or severe eye pain warrants same-day emergency evaluation.
Conservative Management
Preservative-free lubricating eye drops (frequently) and gel or ointment at night
Selenium supplementation 200 μg/day for 6 months — shown to slow progression in mild active TED (evidence from selenium-deficient European populations)
Taping eyelids closed at night for lagophthalmos
Elevated head of bed to reduce morning periorbital edema
Prism glasses for diplopia
Smoking cessation — the single most impactful intervention a patient can make
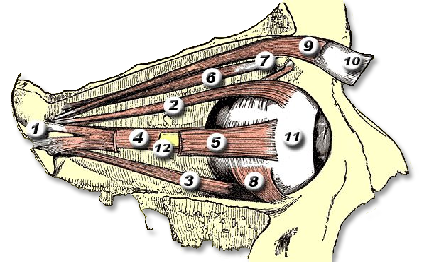
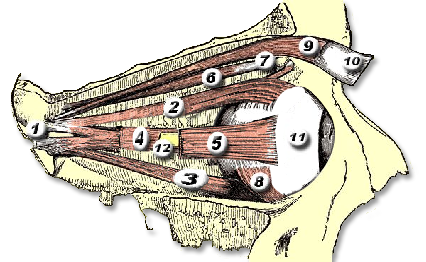
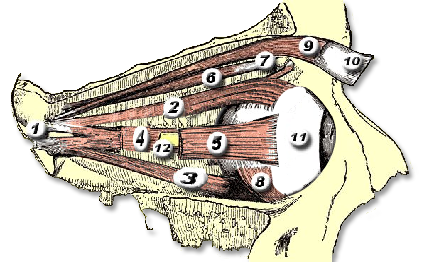
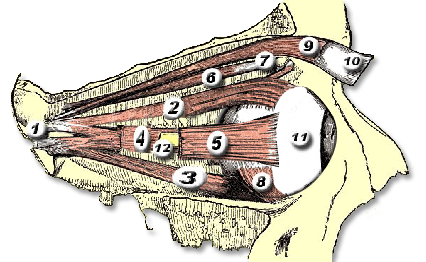
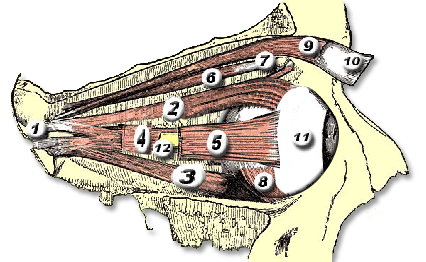
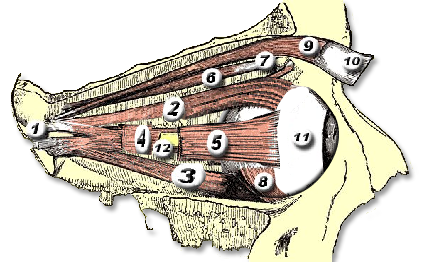
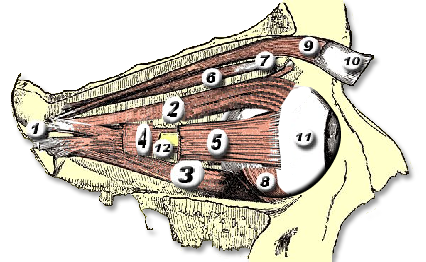
Orbital & Muscle Anatomy
In TED, the extraocular muscles become infiltrated with inflammatory cells, expand due to glycosaminoglycan deposition, and eventually fibrosis. The inferior and medial rectus muscles are most consistently affected, producing the characteristic upward and outward gaze restrictions and diplopia.
Muscle
Primary Function
TED Involvement
Inferior rectus
Depression (downgaze)
Most commonly enlarged — causes hypotropia and limited upgaze; compresses optic nerve at apex
Medial rectus
Adduction
Second most affected — causes esotropia and limited abduction; diplopia on lateral gaze
Superior rectus / levator
Elevation / lid opening
Enlargement restricts downgaze; levator fibrosis and sympathetic Müller muscle stimulation cause lid retraction
Lateral rectus
Abduction
Less commonly enlarged
Superior oblique
Intorsion / depression
Rarely affected
For detailed orbital bone and muscle anatomy, see our Anatomy Overview page.
Frequently Asked Questions
What are the main signs of thyroid eye disease?
Proptosis (bulging eyes), upper- and lower-lid retraction, restricted eye movement with double vision, redness and swelling, and — in severe cases — exposure of the cornea or compression of the optic nerve.
What is the Clinical Activity Score (CAS)?
A 7-point checklist of inflammatory signs (pain, redness, swelling) used to judge whether thyroid eye disease is in its active inflammatory phase, which guides whether medical therapy is appropriate.
Why is an orbital CT scan done?
CT shows the enlarged extraocular muscles characteristic of thyroid eye disease — typically with sparing of the tendon insertions — and helps assess crowding at the orbital apex that can threaten the optic nerve.